
2025 TB Elimination Goal Marred By Low Govt Spending, Erratic Drug & Diagnostics Supply
Only 66% of the required funds for TB elimination allocated over three years from 2017 to 2020

Noida: In 2018, India had said it would eliminate tuberculosis (TB) by 2025, five years before the World Health Organisation’s (WHO) deadline, but the Indian government allocated only two-thirds of the money needed as per its own National Strategic Plan (NSP) for ending TB, government data show.
In 2016, a year before the NSP was adopted, India had 211 TB cases per 100,000 population. In 2022, India had 199 cases per 100,000 population, the latest data show. TB elimination means cases should reduce to 44 cases/100,000 population. The programme also aimed to reduce mortality from TB from 32 to 3 per 100,000 population by 2025. In 2022, the rate was 23 deaths per 100,000 people, as per the India TB Report 2024.
The spending on TB care and prevention has increased over four times from the Rs 19.9 billion spent between 2014-15 and 2016-17, found a government response to a Right To Information (RTI) request filed by IndiaSpend. But the government had outlined an amount of Rs 123.27 billion for TB elimination over three years from 2017 to 2020 in the NSP, and allocated just Rs 83.13 billion.
In addition, experts say the priorities of the government should focus more on diagnostics to detect TB early, and on avoiding drug stock outs as discontinuation of treatment can lead to patients developing drug resistance. Patient advocates say there were several instances of drug stock outs across the country, even in 2024; and the programme spent only 2.1% of its budget (Rs 4.34 billion) on diagnostics up to 2023-24.
With nine months to go before the government’s deadline for TB elimination, IndiaSpend takes stock of the programme.
Stockouts persisted despite higher spending on drugs
The shortest treatment regimen for drug sensitive TB includes a six-month course of rifampicin, isoniazid and ethambutol given over two phases - intensive phase and continuous phase. Each patient requires 56 doses of 300 - 900 mg of each of these drugs every day in the first phase (eight weeks) and 112 doses in the second phase (16 weeks, which can be extended to 24 weeks).
These drugs are administered in fixed dose combinations (FDCs), with each tablet containing the three drugs in fixed doses. The FDCs can be a combination of rifampicin and isoniazid (2FDC), rifampicin, isoniazid and pyrozinamide (3FDC) or rifampicin, isoniazid, pyrozinamide and ethambutol (4FDC).
In 2024-25, India purchased 32.6 million strips of FDCs, each containing 28 tablets. The year before, it purchased 10.16 million strips. In addition, India also purchased 4.8 million tablets of rifampicin and 441,270 tablets of isoniazid in 2024-25, both of which are key constituents of the FDCs.
In March 2024, two doctors wrote to the secretary of the Ministry of Health and Family Welfare (MOHFW) about the “Crisis in Availability of ATT drugs in the National TB Elimination Program”. The letter sought to draw attention to the unavailability of crucial drugs in Chhattisgarh (where one of the authors of the letter works) and Rajasthan, Jharkhand, Madhya Pradesh and Maharashtra, Karnataka.
In Bihar, every district audited faced a shortage of at least one drug between 2016-17 and 2020-21, with some short of 17 out of the 26 drugs required for treatment, a CAG report found.
To tide over the shortage of drugs, health centres were using pediatric formulations which are in stock and supplementing with individual drugs and/or reducing the number of days for which doses are issued at each visit, noted the letter.
“The situation with regard to medicines for drug-resistant tuberculosis is said to be even worse. There are reports of serious interruptions in laboratory reagents especially for molecular diagnostics but even in microscopy,” said the letter.
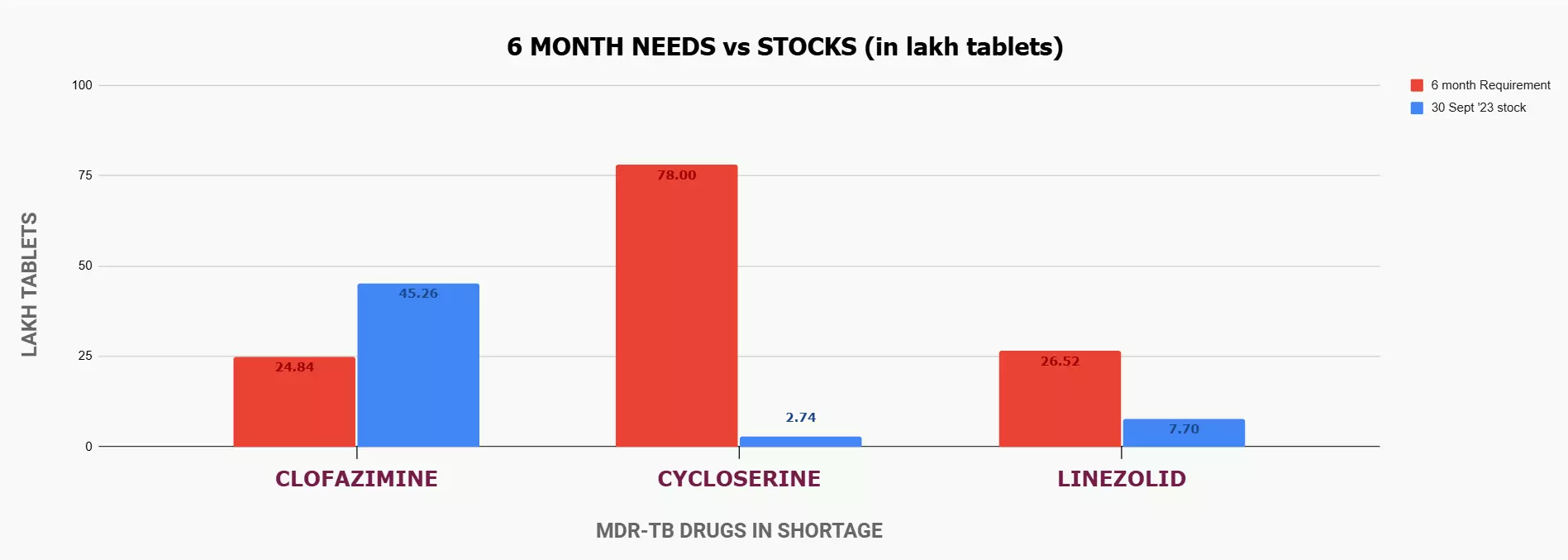
There were 63,929 diagnosed cases of multi drug-resistant TB (MDR-TB), which is resistant to two or more of the commonly used TB drugs, in 2023 in India. MDR-TB treatment uses a combination of drugs such as bedaquiline, delamanid, linezolid, moxifloxacin, fluoroquinolone, pyrazinamide, levofloxacin and pretomanid among others.
India had bought 6.9 million doses of linezolid in 2020, and after three years it procured 5.29 million doses in 2023, and another 6.1 million in 2024.
On September 30 that year, India had 0.7 million doses of linezolid, when the six-month requirement was 2.65 million, as per data compiled by survivors against TB. The following year, it bought 6.1 million tablets of the drug, revealed the RTI. However, there was still another stockout six months later in March 2024, as pointed out by the doctors in their letter.
{kind=link}
India spent Rs 51.45 billion on drug procurement–a quarter of the total amount allocated for the National Tuberculosis Elimination Programme (NTEP) between 2014-15 and 2023-24. But this expenditure was still not enough to streamline the process of drug procurement and avoid stockouts, according to experts.
“Stockouts of TB drugs are not because of inadequate funds allocated but because tenders are not processed in time,” explained Leena Meghnaney, an advocate who works on pharmaceutical policy and was part of Médecins Sans Frontières (MSF) Access campaign, which provided drugs to TB and HIV patients.
States are asked to procure drugs locally in the event of a stockout. However, this is not a good idea, according to Dr T Sundaraman, a member of the coalition ‘India against TB’ and one of the authors of the letter.
“It is difficult for states to negotiate TB purchase in the market and assure quality. I think the TB programme needs to centralise the procurement. They can always rate-contract it and make sure that the drugs are supplied directly to the states and take requirements from the state,” he added.
IndiaSpend has written to the CTD to ask about the expenditure under heads other than drugs and test cartridge procurement, stock of drugs in the country at present, the estimated quantity of each anti-TB drug and test kits required in a year and the number of test cartridges bought between 2014-15 and 2024-25. This story will be updated when they respond.
Low government spending on diagnostics
On December 7, the Minister of Health and Family Welfare announced the commencement of the 100-day campaign to end TB. Increasing the screening for TB is one of the goals of the programme, which aims to accelerate the pace of TB detection and treatment.
The amount set aside for the NSP was to be spent on buying new cartridge-based nucleic acid amplification test machines, establishing laboratories, conducting more tests, managing the existing case load, etc. Additionally, a sum of Rs 7.5 billion was to be spent on tests for patients in the private sector. But the programme spent only 2.1% of its budget (Rs 4.34 billion) on diagnostics up to 2023-24, the RTI shows.
In the ten years between 2014-15 and 2024-25, the government spent only Rs 10.59 billion on procuring diagnostic tests, of which Rs 62.47 billion was spent in 2024-25, per the RTI response.
Some districts in Bihar did not have facilities for several needed TB diagnostic tests in 2020, a CAG report found.
In a reply placed before the Lok Sabha in February 2025, the government said that the procurement procedures and systems have been established to ensure regular and uninterrupted supplies for all consumables required for TB screening and diagnosis.
To fulfil the NSP’s objectives, the government had said it would decrease its reliance on smear microscopy and switch to the more reliable NAAT machines to detect TB cases.
Increasing the procurement of the TruNAAT cartridges, which are manufactured in India, would help increase the testing rate, recommended the 149th report of the Parliamentary Standing Committee on Health in 2020.
However, according to the India TB Report 2024, only about 26.2% of all tests conducted were NAAT, while the remaining were performed using smear microscopy, which is the same technique used by Robert Koch in 1882.
Dated though it may be, microscopy provides results almost immediately within a primary health centre, unlike molecular tests which are conducted at the district level and require up to a week for the results, said Sundararaman. Molecular tests however are more suitable for diagnosing pediatric TB and increasing the use of molecular tests will make it easier to diagnose drug resistance, although the protocol demands that anyone with a confirmed diagnosis be tested for drug sensitivity, he explained.
“I think we should not prematurely withdraw from a technology until a transition is made in a way that requires not just installation of machines and training of more people but ensuring a continuous supply of reagents and cartridges and then setting up domestic manufacturing for the inputs,” he added.
Manpower and infrastructure shortage across states
India’s TB programme is also impacted by manpower and infrastructure shortages.
As of 2024, three states reported vacancies in the TB programme, but over the years several states have had manpower shortages.
Shortages of manpower and low expenditure made the implementation of NTEP deficient in the State of Andhra Pradesh, making the elimination of TB by 2025 uncertain, noted a CAG report. Around 12.1% of all posts in the NTEP in AP were vacant, which was reduced to 10% after the state government accepted the report in August 2023.
A similar audit in Bihar revealed that during the year 2020, all the sanctioned posts (38) of public private mix (PPM) coordinator, who are in charge of coordinating between private organisations working in TB care, the public sector and patients, were vacant across 38 districts and only 158 (29%) of the sanctioned positions (538) for senior treatment supervisors (STS) were filled. The government replied that the PPM posts were still vacant, STSs were supervising more than one district at a time and that drugs would be locally procured to tide over the shortages.
Similarly, Uttarakhand utilised only 59% of the funds allocated under the RNTCP/NTEP between 2016-17 and 2021-22 because funds sanctioned for the State level Lab and Nikshay Poshan Yojna could not be spent. The state TB sanatorium had too few beds, inadequate doctors, nurses and paramedical staff, no CT scan machine and was being run out of a building in poor condition, noted the audit.
In Maharashtra, 74% of the positions for doctors for TB were vacant, as of March 2023. Around 8% of contacts of TB patients, who are at high risk for contracting TB themselves and spreading the infection further, were not tested for TB in 2022, and only 59% of the children who were eligible for receiving preventive TB therapy received it in 2022. The joint director blamed the shortfall on the low supply of isoniazid in 2019-20,refusal by patients and reluctance of private providers to offer preventive therapy. About 79% of the notified TB patients received the Nikshay Poshan DBT in 2022, which the government blamed on the delay in accessing bank account details of the patients.
In Odisha, there were not enough doctors, lab assistants or TB officers. The most that the state utilised from its NTEP budget in any year between 2016-20 was 83%, and the lowest was 39%, found the audit.
In Haryana, some 1,018 patients’ treatment outcomes were erroneously listed as “treatment complete”, making the data on TB treatment rate questionable, and the state TB hospital in Hisar which was declared condemned by the public works department in 2015 was still working.
“The problem is that you can give money to TB but if your overall staffing is low, the facilities are weak, without parallel health system strengthening, you cannot spend the money because you need health workers, community engagement activists, etc. The major reason for underspending is that we sometimes don’t have the human resources to run the program,” said Sundararaman.
‘Catastrophic’ TB spending
The NSP also said it would ensure that no family suffers financially as a result of TB. Though there is no countrywide data for this indicator, information on health spending shows otherwise.
More than 45% of patient families suffer catastrophic expenses while seeking care for TB in India, found a paper by the Indian Council of Medical Research, as we reported in December 2024. To aid the families and the patients themselves with their recovery, the Ministry of Health and Family Welfare provides Rs 1,000 per month to every TB patient under the Nikshay Poshan Yojana.
About 17.23% of patients in Chhattisgarh did not receive the benefits of the NPY, the CAG had found in 2024.
IndiaSpend has reached out to state TB officers in the above states for comment on the observations made in the CAG reports. This story will be updated when they respond.