
In India's Suicide Country, Catching Mental Illness Before It Is Too Late

Farm widows Baby Kinake (left) and Shobha Vetti (right) with their local mental health activist, Shobha Kinake (extreme right), in Mangurda village, Yavatmal, Maharashtra.
Yavatmal, Amravati, Nagpur, Mumbai: Baby Kinake, 39, did not recall anything odd or amiss in her husband’s behaviour in the days before he took his life 12 years ago.
Her husband, Shatrugan, a cotton farmer responsible for a joint family of 10 members in the adivasi (or tribal) village of Mangurda in eastern Maharashtra’s Vidarbha region, showed no change in mood and spoke to everyone politely. No one, least of all Baby Kinake, had an inkling about the stress he was under that would make him, one day in 2007, walk to his fields and swallow poison, leaving his young wife to take care of their two children and their debts.
It was only after Shobha Kinake, a volunteer health worker in Mangurda, started counselling Baby Kinake a few years ago, that she understood how hidden depression might have led Shatrugan to take his life. If she had known what to look out for, she feels, she would have helped him in some way.
Shobha Kinake, 40, is a vital player in efforts to curb mental illnesses in these rural communities, undertaken partly by the Maharashtra government and by a collection of NGOs in the Vidarbha region. It’s an effort prompted by Vidarbha becoming infamous for farmer suicides but also extending broadly to women, non-farmers, adolescents, and young adults.

Shobha Kinake, a volunteer mental health activist, meets and counsels people in her village of Mangurda, Yavatmal, everyday.
Across Maharashtra, 1,300 farmers died by suicide between January and June 2019, the Deccan Herald reported in September 2019. In Vidarbha’s Yavatmal district alone, 139 farmers died by suicide this year, according to government data recorded till July 2019.
The government has launched the Prerna Prakalp Farmer Counselling Health Service Programme and bulked up the existing District Mental Health Programme (DMHP) to address mental illnesses that may play a part in farmer suicides or trouble families generally. They rely on local volunteers like Kinake who have been trained as counsellors and go from village to village to make sure help is at hand.
Under Prerna Prakalp, started in 2015 in 14 of the state’s 36 districts, accredited social health activists (ASHAs), i.e. women who volunteer with the state government to work as local health workers, were trained to detect common signs of mental illnesses through a 12-question survey.
Signs of distress
Is a person eating well, sleeping well, able to concentrate on tasks, and talking to friends and family? Is a person overly worried about crops or finances? Is a person becoming withdrawn and isolated?
The higher the number of negative responses, the more likely that the person needs help, said Sadhna Tayade, director, health services, Maharashtra.
If the ASHA worker becomes concerned about someone, she calls the state’s 104 helpline to reach a team of trained counsellors. Based on the severity of the signs, she may refer a person to a medical officer at the primary health centre or to a psychiatrist at the district hospital.

Anita Jangarmade, an ASHA in Matharjun village in Yavatmal, has to survey villagers for the Prerna Prakalp programme on a daily basis.
To ensure that medical staff are available to deal with her referrals, the DMHP mandates the presence of a psychiatrist with a staff of clinical psychologists, psychiatric social workers, and psychiatric nurses in each district. The programme started in 1997 in the Raigad district but was expanded to 34 of the state’s 36 districts last year. Under both programmes, psychiatrists are required to hold monthly camps in each tehsil of their district.
Like an ASHA, Kinake spends the first half of every day visiting families in Mangurda. Unlike an ASHA, however, Kinake doesn’t just refer patients to counsellors or psychiatrists; she counsels them herself when possible. “I tell families not to refer to mental illness sufferers as paagal (mad),” said Kinake. “I have to tell them not to laugh at them or get angry with them.”
Instead of paagal, villagers are taught to say ‘maansik tanaav’ (mental illness). The term “mentality ka patient” has slowly penetrated in villages scattered across the districts, chipping away at deep-rooted stigma.
Since what she alone can do is limited, Kinake has trained various kathjis (caretakers) within families. Twenty-year-old Geeta in Mangurda, whose mother Jija suffers from schizophrenia, is in charge of her well-being. Jija’s schizophrenia manifested itself three years ago after her brother moved out of their home to stay with other relatives in another village. She asked for him constantly.
Eventually, she stopped eating and sleeping and started walking around the village half-naked. After being trained by Kinake, Geeta ensures her mother eats, sleeps, bathes, dresses, and is involved in a few households tasks. “I try not to let her feel alone,” said Geeta. “I'm always with her.”
Dead chickens to modern medicine
Roughly 30 km from Geeta and Jija’s house, in Kundi village, Bappu Rao Pinder, a cotton farmer bent and wizened with age, credits volunteer Surekha Vikhal Choudhury for teaching him to take care of his schizophrenic son.
Eight years ago when Pradeep first fell ill, he used to lash out at his father, wander the streets at night and pick fights with people. Pinder took him to a local faith healer. He even sacrificed chickens on his instructions. When his son’s condition didn’t improve, he went to private clinics in Yavatmal even though the town was too far for regular visits for treatment.
This continued for two years until he met Choudhury who was also part of the village's family support group, in 2013. She explained the nature of schizophrenia to him and encouraged Pinder to visit the monthly tehsil camp so that Pradeep could get a regular supply of medicine.
On medication, Pradeep is no longer angry and violent. He doesn’t run away from home in the middle of the night and is now able to work in the family’s fields, growing cotton and sorghum.

In Kundi village, Yavatmal, cotton farmer Bappu Rao Pinder is thankful that volunteer mental health activists taught him how to take care of his schizophrenic son.
Apart from the government’s programmes, several NGOs in the area are also active in mental healthcare to supplement the state’s initiatives. For example, the VISHRAM programme led by two NGOs--Prakriti, based in Nagpur and Sangath, based in Goa--which helped farmer Dinesh Ingole who lives in Ghatladki village in Vidarbha’s Amravati district, 165 km west of Nagpur.
Ten years ago, when Ingole first fell ill, he started wandering outside his home, suspecting everyone of bad-mouthing him, picking fights with his family, and insulting people on the streets.
Ingole’s ties with his friends and neighbours frayed. They saw him as mad and dangerous. As he sank deeper into his illness, he became physically weaker and unable to work. His family struggled with expensive private doctors in Amravati till a local mental health volunteer, Syed Younis, enlisted the help of VISHRAM--Vidarbha Stress and Health Programme--in 2014. With medication, counselling, and a more understanding family, Ingole is slowly getting back on his feet.
Catching mental illness early
It’s the goal of the government programmes and of the NGOs working here to catch mental illness early and treat it. The will is there but often what is missing is adequate staff and infrastructure.
For example, the district hospitals where psychiatrists are posted are often a long way away, making regular visits by patients difficult. Mangurda in the Kelapur tehsil, close to the Telangana border, is 70 km from Yavatmal town where the hospital with the district psychiatrist is located.
Data from Tayade’s office, recorded up to August 2019, show that four of the 14 positions for psychiatrists under Prerna Prakalp are currently vacant. It’s not just psychiatric professionals; the lack of personnel extends to local-level workers.

“Around 60% of the posts in government programmes are vacant. We’re trying to train people from the community level to address this problem of human resources,” said Tayade.
Of the 60,000 ASHA workers in the state, less than half have been trained under Prerna Prakalp. Just 45.48% of ASHAs were trained for mental healthcare from April 2018 to August 2019, according to the state’s data till August 2019. In 2015-16, which was Prerna Prakalp’s first year, 20,185 ASHAs worked under the programme; four years on, the number of ASHA workers under Prerna Prakalp has increased only by 740.

Training for personnel under the DMHP too remains inadequate with 45.36% of ASHAs, 34.57% of paramedical staff and 48.39% of medical officers being trained, according to the state data.

Forty six sessions were held in the 34 districts from April to August 2019 to screen farmers in particular. Of the 2,079 farmers who attended, 261 were diagnosed with mental illness and treated according to the DMHP protocol. In addition, there were 282 sessions for school children, where 298 were treated; 103 sessions for the elderly where 394 were treated, and 96 for prisoners, where 1,390 were treated. Getting hold of farmers is the hardest. The DMHP staff have to wait for them till evening when they have finished their work in the fields. Sometimes, they have to go looking for them to convince them to attend these screenings.
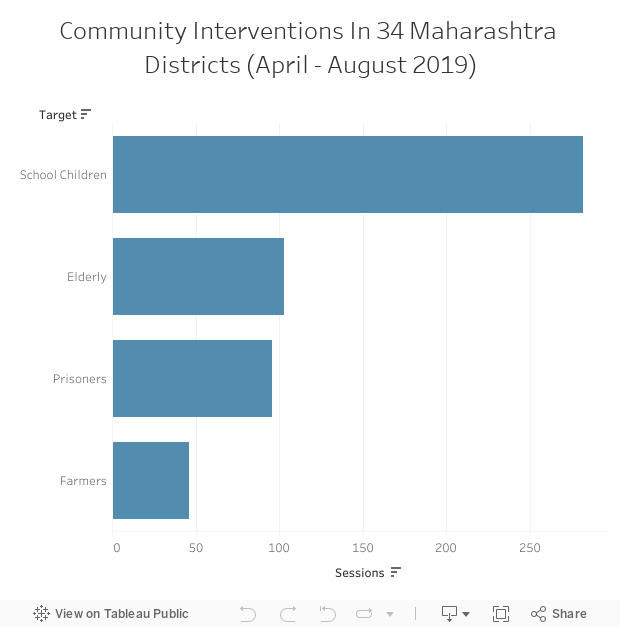
>Source: Data shared with IndiaSpend by director, health services, Maharashtra
The challenges of network building
While VISHRAM ran in 30 villages in Amravati, over 18 months between 2014 and 2015, other NGOs also pitch in with their own mental health projects. Choudhury and Kinake are attached to the Society for Rural and Urban Joint Activities or SRUJAN, based in Nagpur and in Mangurda, which has 12 mental healthcare activists spread across Yavatmal.
The organisation had been working on maternal and child healthcare in Yavatmal since 2000, when it realised that the infants they had helped were growing into adolescents and young adults with depression. SRUJAN aims to create a network of community health workers who can step in when ASHAs find themselves stretched too thin.
“The government needs to understand community-based welfare,” said Ajay Dolke, who co-founded SRUJAN. “The support for mental illness sufferers must start with the family and neighbours. They have to be counselled on how to provide care. If one needs to visit a psychiatrist, his neighbour should step in to say that he'll manage the former’s field or cattle for the day. This only happens when people recognise that mental illness is, indeed, an illness.”
The NGO activists feel they are better trained than ASHAs. They devote their time not just to sufferers but also with the caretakers and with the bereaved who have lost loved ones to suicide. They battle superstition and stigma around mental health and change the very language used to talk about sufferers. In Yavatmal, the family support groups--started with the help of SRUJAN--give caretakers space to talk about their burdens and get support.
Abhishek Mamarde, a psychiatrist with the Nagpur district hospital, trained volunteers in Ghatladki and Asegaon villages for VISHRAM. “We had to train volunteers to listen, to not be harsh, and ask open-ended questions about what people think of their lives and what they want to do with them,” he said.
Volunteers have to pick up the fact that the near-universal use of the blanket word ‘tension’ can mask a host of illnesses such as severe anxiety or depression. Zahir Saudagar, 40, a farmer in Ghatladki village, Amravati, began suffering terrible headaches a few years ago in the midst of a drought when he had to pay for four family weddings. Everyone kept saying he was suffering from ‘tension’. “I felt a heaviness all the time. My heart and my body were heavy. I was scared I would get a big illness,” he said.
It isn’t just failing crops and loans that plunge villagers like him into despair, it’s also failing to meet aspirations such as providing for the family or paying for weddings. Saudagar felt permanently miserable because he felt he was failing those around him. Counselling by VISHRAM made him understand that the cause of his headaches was anxiety. The programme’s results showed the number of people with depression who sought care rose from 4.3% to 27.2% in the 18-month period.
The burden of responsibility
Despite the training and sensitisation, community social workers, volunteers, and ASHAs worry about the immense responsibility placed on them.
ASHA Anita Jangarmade, 32, meets families in Matharjun village, Zari Jamani tehsil every day. Her register, with responses to the 12-question survey on mental health, is evidence of her rounds. Yet, she frets over the ‘yes’ and ‘no’ responses that she records in blue ink.
One-word answers tell her little about a person’s state of mind and leave her open to blame should there be a suicide among one of her charges. “If someone’s thoughts do go in that direction, or if he had a fight at home and drinks pesticide, then how can I prevent him from dying?” she asked.
They also face villagers’ anger when psychiatrists are not at their post. In Yavatmal district where large swathes of forested land make for unreliable phone networks, there is no way to find out whether psychiatrists are present in district hospitals and at the monthly tehsil camps. If they fail to show up on their scheduled days, “it shakes people’s faith in us”, said Kinake who has faced the wrath of people who travelled long distances only to find no psychiatrist.
The lack of availability of medicines for severe mental illnesses at pharmacies in tehsil towns is another sore point. No local NGOs or private organisations are allowed to stock in bulk ‘Schedule H’ drugs which cannot be purchased over the counter. Caretakers and sufferers are invariably forced to undertake a trip to Yavatmal to procure medicines. Many go without medication for months, worsening their condition.
Officials like Tayade are aware that all these issues require a coordinated response from all the concerned departments in each district, particularly to fill the current vacancies. One measure, mandated by the central government, that may, albeit only in the long term, help create trained manpower, is the plan to turn three of the state’s four mental hospitals in Thane, Pune, and Nagpur into Centres for Excellence. This will result in more seats for psychiatry, clinical psychology, psychiatric social work, and psychiatric nursing from next year.
This reportage was supported by the Thakur Family Foundation. The Thakur Family Foundation has not exercised any editorial control over the contents of this reportage.
(Wal is an independent journalist based in New Delhi.)
We welcome feedback. Please write to respond@indiaspend.org. We reserve the right to edit responses for language and grammar.
